



SWI – Susceptibility Weighted Imaging for MRI after TBI
SWI – Susceptibility Weighted Imaging – Best Hemosiderin Tool
Call me at 800-992-9447
SWI “Susceptibility Weighted Imaging” (“SWI”) picks up where gradient echo imaging stopped. Every few years, I get excited again about some advance in neuroimaging to help prove the mild brain injury case. Diagnosing concussions involves reconstructing evidence of what happened in a medical event, were the overt syptomatic evidence is transient. Thus, the ER doctors are too reliant on getting history of what happened from someone who likely has memory problems of what happened. In fact, the memory problems are the best evidence of concussion. Yet, if you ask the question the wrong way, you don’t get evidence of memory problem, you just get no evidence.
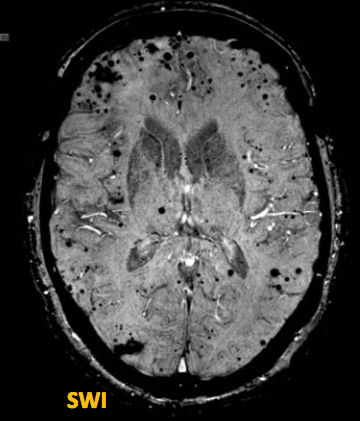
SWI image. Pathology is shown where the deep black holes appear on this scan. This scan is used for demonstrative purposes as it has far more pathology than would be seen on a post-concussion scan.
Thus, the quest for the Holy Grail for a bright line tool to prove concussion is ongoing. SWI is the most tangible of the new MRI techniques to prove a mild brain injury, even though it is abnormal in fewer cases than other developments such as DTI. On our previous page, we discussed the hemosiderin traces brain bleeds leave behind. Ten years ago, GRE (gradient echo imaging) was the state of the art in imaging those hemosiderin stains. Yet in an overwhelming percentage of MTBI cases, the GRE was normal. Gradient Echo Imaging was to be the breakthrough technology. It has had little value in MTBI cases.
SWI is searching for the same thing as GRE but is a huge leap forward because it is five times more sensitive than GRE. SWI tunes the magnet to detect microhemorrhages where conventional MRI cannot. Like Gradient Echo Imaging, it images the hemosiderin staining on brain tissue. [1] The puzzle is whether five times better is enough when you may be talking about multiplying zero. If no hemosidrin deposits show up in even complicated MTBI cases, it may very well be that the kind of bleeds that leave hemosiderin behind are not the principal culprit in the MTBI. Time will tell.
The exciting part of an abnormal SWI in a post-concussion case is that almost anyone can tell what they are looking at on a SWI image. Lesions on conventional MRI are fuzzy and small, with the contrast color between the whiter gray of lesion versus the darker gray of the surrounding matter, difficult to see. It is even harder to see such abnormalities when shown on a projector in a well lit room. Radiologists work on high resolution monitors in dark rooms. But with SWI, the abnormalities are a dark black. There is no mistaking the dark black holes shown on the SWI to the right.
Of course the SWI image to the right is not a MTBI scan. Still, even three to five holes comparable to the smaller holes shown on this scan, would show significant pathology in a MTBI. So in the cases where the SWI is abnormal, it should be a simple matter to show that to demonstrate that pathology on the scan.